Fetlock Lameness
– It’s importance and how MRI can assist in making the difficult diagnosis
Dr Robin Bell and Professor Leo Jeffcott
Equine Performance and Imaging Centre,
University of Sydney Veterinary Teaching Hospital Camden.
Lameness involving the fetlock joint is an all too common problem in performance horses and racehorses. Injuries to this region may involve the joint itself or the surrounding soft tissues, and are often determined by the use of the horse. The fetlock is a complicated high motion joint that is always subjected to huge forces and stresses during locomotion. The classic movie pictures of the American photographer Eadweard Muybridge taken over 120 years ago (pictured above) clearly show the degree of extension of the fetlock during galloping in the horse. The structures most commonly damaged in fetlock injuries are illustrated.
The good news is that many fetlock problems are fairly simple to diagnose. As we have described in the previous two articles, lameness can be localised to the fetlock by careful clinical examination (i.e. palpation), evaluation of gait (especially under saddle), response to flexion tests (figure 3) and nerve blocks or desensitisation of the joint itself.
FETLOCK DISORDERS
A full list of the potential causes of fetlock lameness is shown in Table 1, but there are three broad categories of conditions that can affect the fetlock:
1) Acute or repetitive injuries that do not involve a fracture, these include osteoarthritis, inflammation within the fetlock joint itself (synovitis, capsulitis) or the ligaments supporting it, and injury to the bones without fracture such as inflammation of the sesamoid bones (sesamoiditis).
2) Fragments within the joint that can be removed surgically via keyhole surgery (arthroscopy) whether developmental (osteochondrosis type lesions) or traumatic (such as chip fractures or small sesamoid fractures).
3) Major fractures involving the joint such as condylar fractures of the cannon bone, or fractures of the long pastern bone.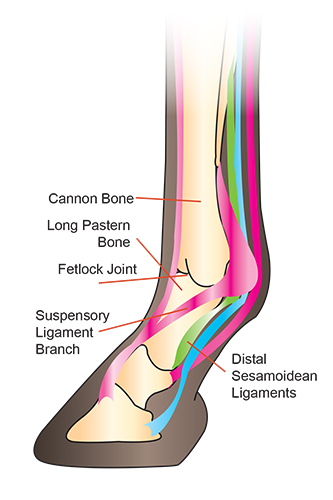
By far the most common conditions affecting the fetlock are those that fall under the umbrella of injuries that do not involve a fracture. The diagnosis of these problems follows the same basic steps as outlined in our previous two articles, with examination by a vet, localisation with nerve blocks and the use of diagnostic aids. As the fetlock is a high motion joint, even relatively mild arthritis can adversely affect performance. These horses will generally have evidence of disease on x-rays such as bone spurs or flattening of the condyles of the cannon bone, but in early disease the changes may only be visible with MRI. Treatment for this condition involves rest, in combination with joint injections. Low dose corticosteroids in combination with hyaluronic acid (a joint ‘lubricant’) are very effective in controlling the inflammation within the joint and alleviating lameness. Many horses that do not respond to this treatment will respond favourably to intra-articular injection of a product called IRAP®. This product amplifies the horses own, naturally occurring anti-inflammatory mediator which is then re-injected into the joint. IRAP® reportedly shuts down the inflammatory pathway before it starts to do damage to the cartilage within the joint. Regenerative medicine products such as stem cells and PRP (platelet rich plasma) injected directly into the joint are promising new products for the treatment of fetlock joint arthritis, but to date there is no good evidence to show that they are actually efficacious in the treatment of arthritis.
Suspensory ligament branch desmitis
is another very common injury of the fetlock region and is most often seen in horses that compete in eventing, although it can occur in any performance horse. This condition involves a tear or strain of the suspensory ligament where it branches onto the bones at the back of the fetlock joint (sesamoid bones). These tears can be seen on an ultrasound examination, and horses may often have swelling over the affected branch, that may be hot or painful to touch. Suspensory branch desmitis, responds well to rest and controlled exercise. In cases with a discrete hole within the ligament, injection of stem cells, or other regenerative medicine products show real promise in speeding healing, and decreasing the rate of re-injury.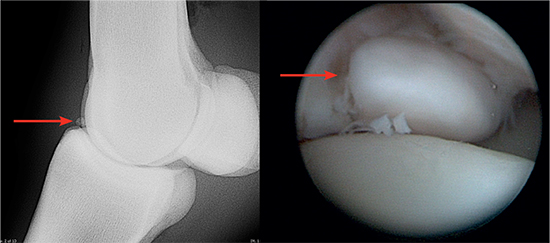
Radiograph showing chip fracture in the fetlock joint of a young racehorse, and the view of the chip at arthroscopic surgery
Chip fractures or fragments within the fetlock joint are generally best removed surgically via arthroscopy. If the chips are within the joint they can cause damage to the cartilage surfaces, and promote inflammation which can lead to arthritis. It is possible to keep a horse in work and sound even in the presence of chip fractures, but this often hastens the onset of osteoarthritis, and may cause the horse to remain lame even if the chips are removed surgically at a later time.
Major fractures involving the fetlock joint are most common in racehorses, although jumping and dressage horses can develop simple fractures of the cannon bone or long pastern bone. These simple fractures can often be repaired very successfully using screws to compress the fracture line and restore congruency to the joint. More serious fractures that have multiple fragments carry a very poor prognosis. Fusing the fetlock joint is an option in these cases, but results in persistent lameness, and animals with a fused fetlock joint are only able to be used as paddock animals.
Straight and oblique sesamoidean ligament desmitis
Injury to the ligaments at the bottom of the sesamoid bones (straight and oblique distal sesamoid ligaments- Fig 2.) in the fetlock is now being recognised as a major cause of lameness particularly in jumping horses. These injuries can be diagnosed on the basis of an ultrasound scan, but this is a difficult region to scan, because of the anatomy of the bottom of the fetlock. Again MRI can help to aid in the diagnosis of such injuries, and may also allow some insight into the progression of healing during the rehabilitation period. The prognosis for distal sesamoidean ligament injury is generally good, given appropriate rest and rehabilitation. As with suspensory ligament branch injuries, injection with regenerative medicine products is showing some promise as a helpful adjunctive therapy in these horses.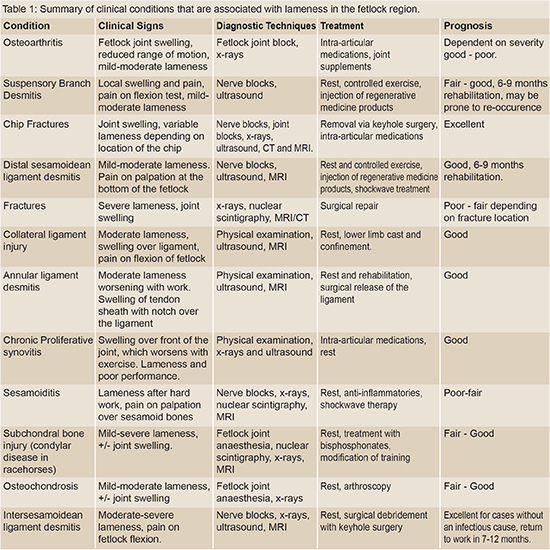
The place for MRI
Unfortunately there are cases where establishing a diagnosis of fetlock lameness cannot be readily achieved with clinical examination, x-rays, ultrasound and nerve blocks. In these cases MRI can be an extremely useful diagnostic tool. What we would now like to do is to inform you of the potential benefits of MRI in three ways; 1) what MRI can detect for us, 2) provide a case report where MRI was essential in making the correct diagnosis and 3) report some preliminary research that will assist future cases of fetlock injury.
Nuclear scintigraphy and x-ray of a horse with a condylar fracture. Arrows indicate the region affected and the fracture line.
1. MRI basics
MRI uses a magnetic field and radiofrequency pulses to generate an image based upon magnetic properties of the hydrogen ions within the body part being imaged. There are many different pulses that can be used to highlight specific tissue types and disease processes, additionally it has the advantage that images can be obtained in any plane or orientation. MRI provides exquisitely detailed soft tissue images and provides information about subtle pathology within joints, tendons and ligaments. This can be of particular use in cases where other diagnostic modalities such as x-rays, ultrasound or bone scan have not provided a specific diagnosis, or more information about the problem is needed. This is allowing us to accurately diagnose, and more effectively treat a wide range of conditions, thus returning these horses to performance faster than without such targeted treatment.
MRI pictures from normal horses’s fetlock (red arrow – cannon bone, white arrow – long pastern bone, blue arrow – flexor tendons). Note the multiple imaging planes and amount of bony, joint and soft tissue definition. Compare these normal images to those in the case report below.
2. Case report using MRI:
A good example of the benefits of using MRI in cases where other more traditional methods do not provide an answer is illustrated below. The horse in question had a lameness that was able to be localised to the fetlock joint with nerve blocks, but there were no significant changes present on x-rays or ultrasound of the region. Medication of the joint with intra-articular corticosteroids and hyaluronate and a period of rest did not improve the lameness significantly. MRI scans of the fetlock showed a very significant area of bone bruising. After a further period of rest, and treatment with a class of drugs called bisphosphonates the horse was able to return to full work without lameness.
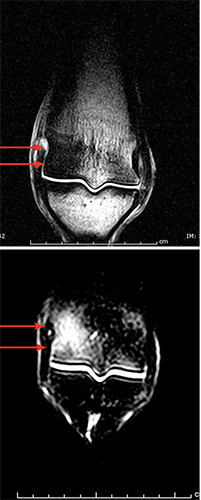
MRI images of the same horse which revealed evidence of significant bone bruising (white area of bone in image (b) as indicated by arrows. This bone brushing can be treated with drugs called bisphosphonates, and generally does not respond to intra-articular medications. There was no evidence of cartilage defects or other joint damage and this horse successfully returned to work.
3. MRI Research
Here at the University Veterinary Teaching Hospital Camden we are using the MRI to investigate this so-called bone bruising in young racehorses (condylar disease), as this often occurs in the condyles at the bottom of the cannon bone, and may be a precursor to catastrophic fractures in that region. If detected early with the aid of MRI these horses can be treated, and return to work without the risk of such a devastating and life threatening injury developing. We have an ongoing project to examine the fetlocks of racehorses that have had to put down for other reasons. We are comparing the MRI pictures with histopathological specimens at the microscopic level, the results of this study will be published in the scientific literature.

Flexion tests and evaluating the horse under the saddle are both important steps to aid in the localisation of lameness to the fetlock.
CONCLUSION
We hope that you will see from the information presented in this article that lameness involving the fetlock region can be caused by a wide range of very different conditions. Although the diagnosis of these conditions is often relatively simple, advanced diagnostic modalities such as MRI or nuclear scintigraphy may be necessary in order to ensure that an accurate diagnosis is reached, thereby maximising the chances of returning your horse to full performance.

Still images taken from Muybridge’s original sequence of photographs to illustrate the individual phases of the gallop. Note the amount of extension of the fetlock in a normal horse at the gallop, with the back of the fetlock almost hitting the ground. This is an excellent illustration of the stresses that this region is placed under in performance horses.
This article first appeared in the May 2011 issue of THM.
Very useful information. My Andalusian filly injured her fetlock joint somehow in her stall. I live in a remote area and will be trailering her to a large equine medical center tomorrow. Your article will help me ask the vet the right questions. I was especially interested to see the MRI scans and how useful they were in pinpointing out specific injuries. Thank you.
I have a horse that is strong and canter however he goes lame at times ( to the point where he is stiff in the left leg) hypertension of the knee almost in a walk and can’t trot / however he seems fine the next day …. I’m very light with him / if he wants to run fine if not I don’t push him …. but it’s sad not letting him run ….. I have therapy boots on him to try to help I took off his shoes and he seemed fine …. it’s just an ongoing problem ( I’m looking for answers ) I’m afraid to get all sorts of tests done when it’s tissue related …. and there is nothing that can be done ( just rest)
Thank you for this article it is very informative as I have a horse that is lame in the front right. we have already done the x-ray. we are doing the wave message to help. I can talk to my vet about this and see what she thinks. I want my horses to stay healthy and what only the best.
I have a horse which will break at the fetlock but so far only at a walk. She also has been evaluated with navicular disease.
Does the navicular have an effect on the fetlock and will it progressive get worse and will she break down at a faster gait?